

Characterized by the breast extending over the chest fold, which often times creates a slight breast roll.

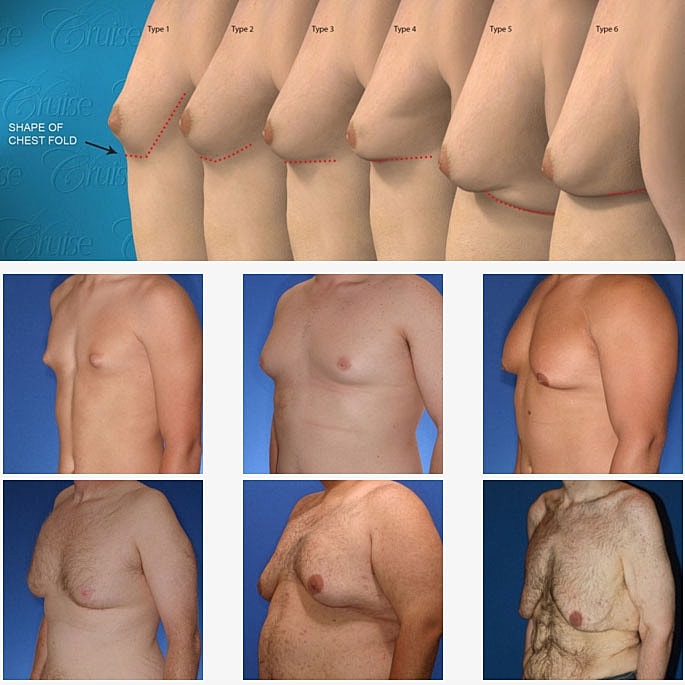
Based on over 2500 gynecomastia surgeries, Dr. Cruise has classified gynecomastia into 6 different types.
Each type is unique in its own way and must be treated differently. The purpose of the Cruise Classification System is to:

A classification system is only useful if it outlines a treatment plan.
Dr. Cruise
Notice the progressive increase in skin laxity. This excess skin will change the type of surgery necessary to properly correct the problem.
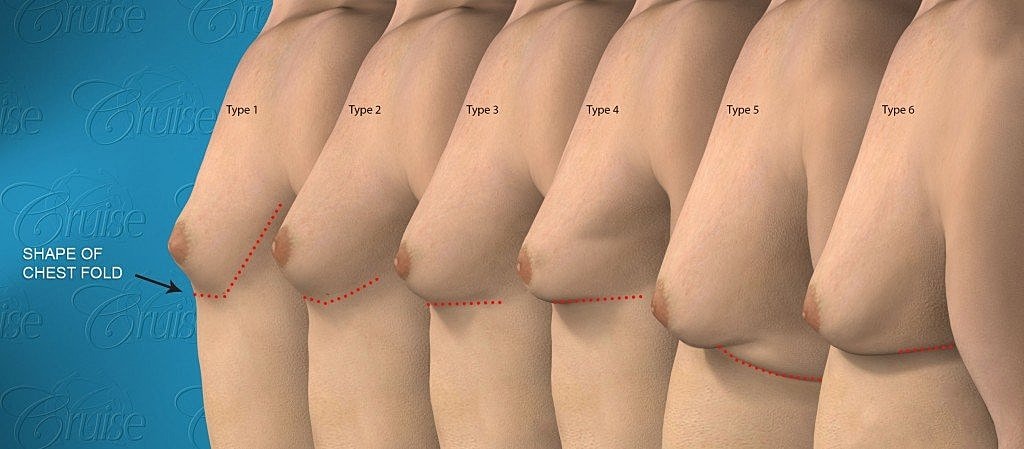






Type 3 Gynecomastia, also known as slight breast roll, has similar breast tissue draping over the pectoralis muscle as Type 2.
The difference is that the skin has relaxed and is no longer able to compress the tissue into a tight, rounded appearance. Instead it takes on a horizontal appearance.
Nipple is at or below the pectoralis border but exact position is not easy to determine because muscle border is blurred by breast tissue. Nipple descent represents moderate skin laxity which shows itself as a horizontal chest fold instead of rounded. The skin is no longer tight enough to wrap around the muscle border.
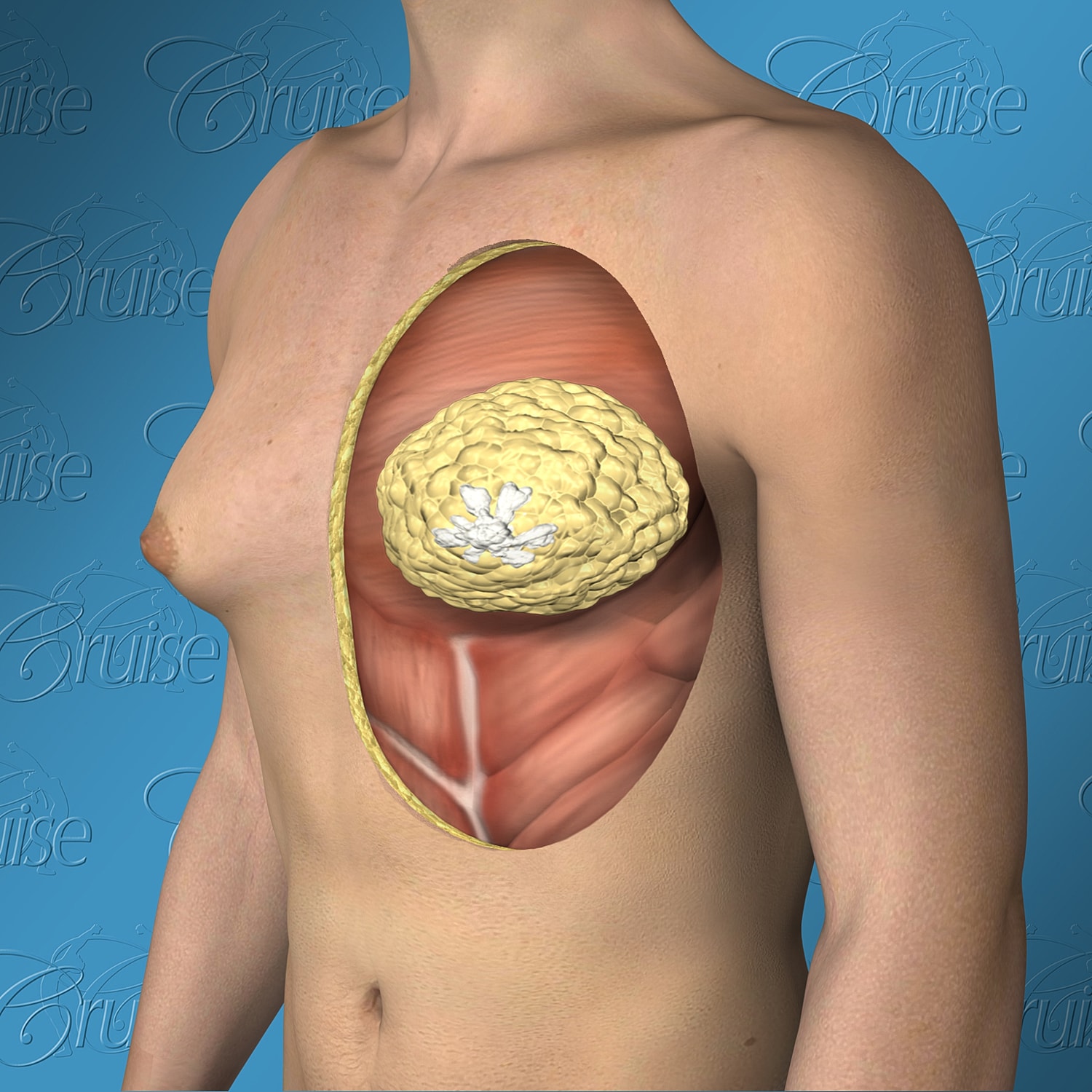
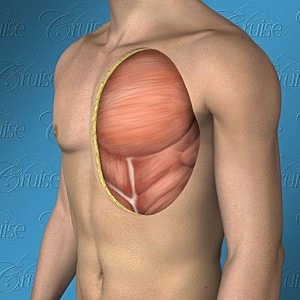
This image demonstrates well how the breast tissue drapes over and blurs the pectoralis muscle border. The amount on the chest in type 3 is usually similar to type 2 but there is usually more tissue that extends into arm pit area. Removing this is critical to define the muscle.
Unfortunately, the clinical definition for optimal results is virtually non-existent; even in plastic surgery literature. This is why it was essential for Dr. Cruise to include it as part of the Cruise Classification System.
A classification system is only useful if it identifies where you are and where you need to go. The first part of the classification system identifies 6 basic types based on where you are. This part of the system identifies where you need to go. It is true, different men have different goals. However, Dr. Cruise’s has identified eight fundamental aspects of the male upper chest that need to be evaluated in order to achieve a masculine chest. These eight components are outlined below.
Optimal results for Type 3 primarily involve 1-4 and to a lesser extent 5 and 6. Addressing these aspects determines your surgical road map. Proper evaluation is particularly true for Type 3 gynecomastia as these are the patients that are just beginning to show moderate skin laxity.
“Achieving optimal results and avoiding complications requires both expertise and a plan”
Dr. Cruise

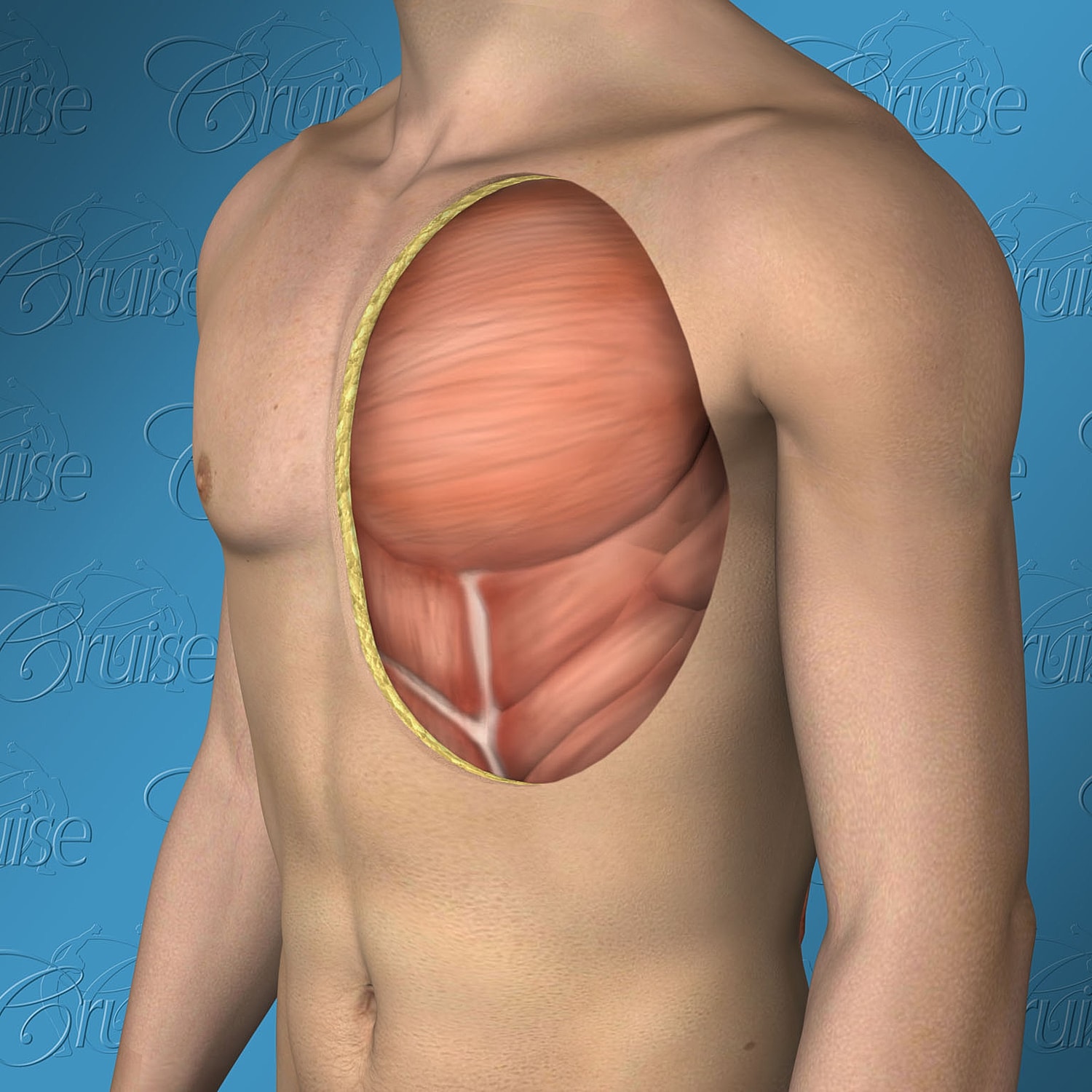
External view of masculine chest
Internal view of masculine chest
The Cruise classification accurately defines “where you are”. Now, we need to clearly define in surgical terms “where you want to go.”
With this is mind, we asked Dr. Cruise to outline the most important aspects that need to be addressed when surgically treating gynecomastia and what they should ideally look like.
Overall, a masculine chest is full and powerful above the nipple but ripped and defined below. The key is to create muscle definition, flatten the nipple, yet keep the chest area above the areola normal thickness. Thinning too much will create a “fragile” appearance and worse, may create contour irregularities. The goal is to flatten the chest so that you can confidently wear tight white T-shirts and to create a V shape from both the back and front view.
Ideally, the nipple should be 1-2 cm above the pec. border (pectoralis major muscle). However, it is perfectly acceptable even if it is located directly on the border as long as it sits on a convex (not concave) surface. This is particularly true with body builders or men with large pec. muscles as it gives the low lying nipple a bigger base to sit on. However, when it sits below the pec. border it begins to face downward or worse it falls into the chest fold which is concave. Sitting in the chest fold often gives the appearance of “cratering.”
The areola is the dark, pigmented skin around the nipple. Areola size is proportionate to chest size. Ideally, it should 25-35 mm and lay flush with the surrounding skin. However, slight elevation is common. Most people do not consciously realize it but areolas are usually wider than they are tall. A perfectly round areola is not ideal and an areola that is taller than it is wide may even appear unusual or “surgical”.
Ideally, the pectoralis major muscle should be defined and straight with the skin wrapping around it into a well defined chest fold and then into a defined arm pit hollow. Excess breast tissue, fat and/or saggy skin will blur this border and create a round, feminine appearance.
Should have sculpted appearance with a well define hollow at its apex. The borders of the pec. major in front and the latissimus dorsi in back should be well defined giving a V shape to the upper body. Excess fat/saggy skin can fill the arm pit creating an uncomfortable fullness in armpit and a saggy breast roll just below. Creating a sculpted axilla and a V shape appearance to the upper body is one of the most rewarding parts of gynecomastia surgery yet it is usually overlooked as not being part of the gynecomastia. It is important for your surgeon to understand that the goal of surgery is to create a V shaped, masculine chest and not just to remove breast tissue. I can not tell you have powerful the results are when you create a sculpted pec., lat. and arm pit. It is truly life changing.
Ideally, there should not be any fat pockets. There are three common fat pockets that need to be evaluated and removed if present:
Should not be present. Not applicable to Type 3.
Not applicable to Type 3
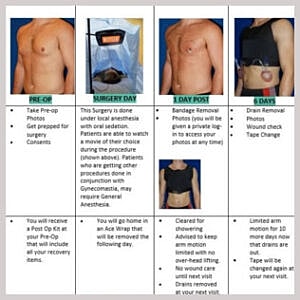
Below you will find treatment options for Type 3 Gynecomastia, along with an explanation of how the result differs for each.
This is often the biggest struggle slight breast roll gynecomastia patients have. Type 3’s and Type 4’s are where incision choices make the biggest difference. Experience has shown time and time again that chest shape trumps incisions with rare exceptions. In addition, it is important to consider how you will look not only in 1-2 years but also in 1-2 decades and beyond. Any skin laxity now will be a real problem as you age while incisions will be little more than a faded memory. It is better to have time on your side.
Crescent excision means that a 1/4″ to 1/2″ crescent shaped piece of skin is removed just below and above the areola. This does several good things beyond tightening the chest skin. More importantly, it pulls the areola tight similar to getting the wrinkles out of a bed sheet. This little maneuver has a large impact in getting rid of excess skin that has been stretched over time. It also flattens the lower and upper chest skin mildly so that it better wraps around the pec. border improving definition. One incision is located above and second below the areola.
Crescent incisions, however, create skin margins that do not line up exactly. The side toward the areola will always be shorter than its counterpart. When sutured together this length mismatch will create mild bunching that takes a little longer to fade away than a linear incision would.
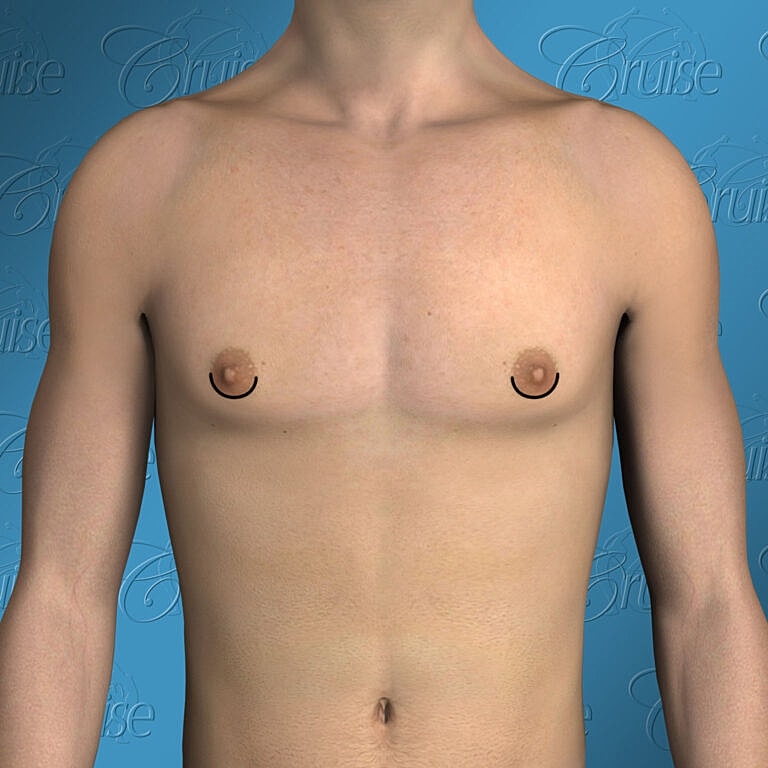
Inferior crescent excision means that a 1/4″ to 1/2″ crescent shaped piece of skin is removed just below the areola. This technique not only tightens the chest skin, but, more importantly, it pulls the areola tight similar to getting the wrinkles out of a bed sheet. This little maneuver has a large impact in getting rid of excess skin that has been stretched over time. It also flattens the lower chest skin mildly so that it better wraps around the pec. border improving definition. The incision is located low on the areola where it is very hard to see even early on.
The superior incision is used to slightly elevate the nipple to make sure it stays on the convex pec. border and does not migrate downward into the concave chest fold when the breast tissue is removed. If this occurs and it could create a “crater” appearance. This is very common with Type 3. While a super incision is good from a positional standpoint, it does create some additional tension on the incision which means it will take longer to fade. Overall, it is the optimal option for lower hanging nipples.
Dr. Cruise does not use a full circular incision around the border of the areola (a.k.a. donut incision, donut lift) because it can create a puckered looking nipple. With the superior and inferior incision there is a break/gap between them for the purpose of avoiding this issue. Crescent incisions, however, create skin margins that do not line up exactly. The side toward the areola will always be shorter than its counterpart. When sutured together this length mismatch will create mild bunching that takes a little longer to fade away than a linear incision. For that reason a third incision is introduced, a small vertical component that fades very well. It get’s rid of the mismatch and also tightens the skin horizontally.
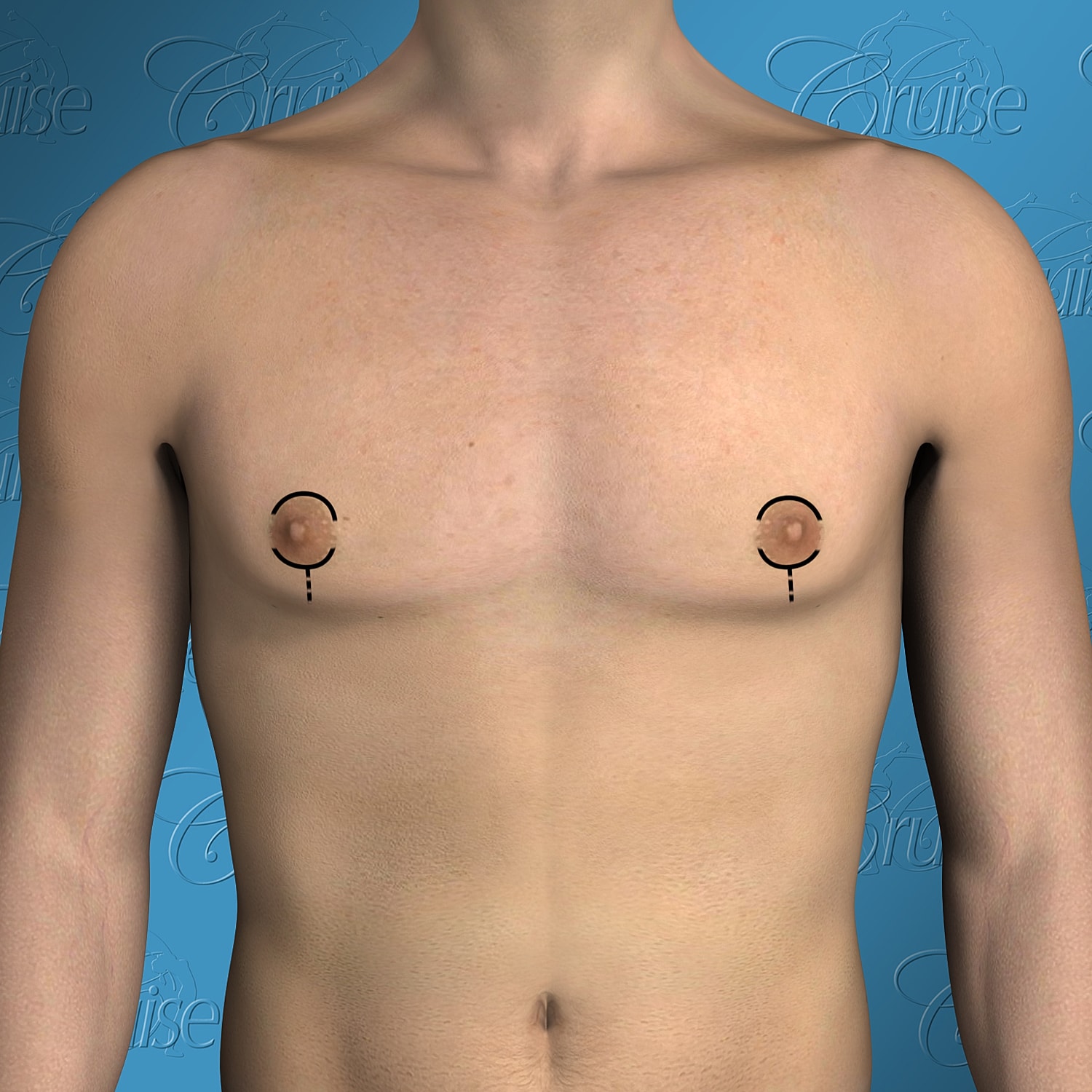
Inferior crescent excision means that a 1/4″ to 1/2″ crescent shaped piece of skin is removed just below the areola. This technique not only tightens the chest skin, but, more importantly, it pulls the areola tight similar to getting the wrinkles out of a bed sheet. This little maneuver has a large impact in getting rid of excess skin that has been stretched over time. It also flattens the lower chest skin mildly so that it better wraps around the pec. border improving definition.
The incision is located low on the areola where it is very hard to see even early on. The superior incision is used to slightly elevate the nipple to make sure it stays on the convex pec. border and does not migrate downward into the concave chest fold when the breast tissue is removed. If this occurs and it could create a “crater” appearance. This is very common with Type 3. While a super incision is good from a positional standpoint, it does create some additional tension on the incision which means it will take longer to fade. Overall, it is the optimal option for lower hanging nipples. Dr. Cruise does not use a full circular incision around the border of the areola (a.k.a. donut incision, donut lift) because it can create a puckered looking nipple. With the superior and inferior incision there is a break/gap between them for the purpose of avoiding this issue. Crescent incisions, however, create skin margins that do not line up exactly. The side toward the areola will always be shorter than its counterpart. When sutured together this length mismatch will create mild bunching that takes a little longer to fade away than a linear incision. For that reason a third incision is introduced, a small vertical component that fades very well. It get’s rid of the mismatch and also tightens the skin horizontally.
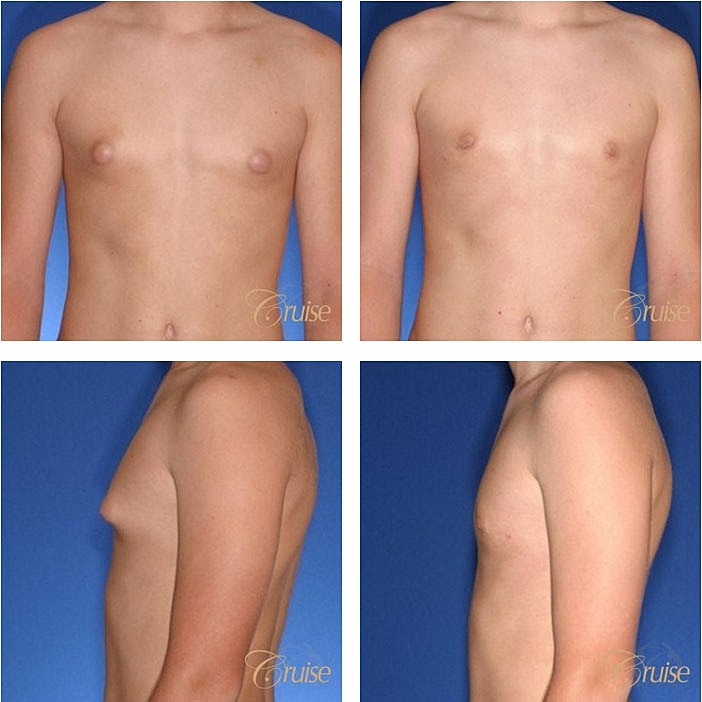
View our gallery of before and after photos to see the results from slight breast roll Gynecomastia surgery. Remember, each patient is unique and results will vary from patient to patient.
1 of 2


The pain and suffering associated with gynecomastia is unlike any other condition in plastic surgery and perhaps in all of medicine. The range of its impact is stunning. Some men (usually older) can be relatively unaffected while others (usually the younger) can be completely devastated and even suicidal.
Unfortunately, because of the stigma associated with it, it is not always readily apparent what your loved one may be experiencing. In fact, the men or more commonly pubescent teenagers, who are most deeply affected go to great lengths to suffer alone. The Internet becomes the only one they can talk to. This dangerous combination of deep emotional pain and isolation makes them particularly vulnerable to exploitation. Exploitation that takes the form of the literally thousands of “miracle” cures that have no medical merit to the more nefarious types looking to take advantage of the the emotionally weak.
Wide spectrum of outward expression from normal to:

Gynecomastia surgery is a tangible next step to resolve your man boobs. Dr. Cruise has performed over 5,000 gynecomastia surgeries and is ready to see you for a consultation. Call us at 949-644-4808 or fill out our online contact form and you will be contacted with the next steps!